

During the past ten years, I traveled to over 100 jails and prisons in the entire east coast of the United States, giving me the to opportunity to observe the dire lack of appropriate medical and mental health care in our prison system. The most immediate and urgent need is to screen routinely for Post Traumatic Stress Disorder (PTSD) among incarcerated individuals.
 After assessing over a thousand men who face lengthy prison sentences and endured long periods of solitary confinement, almost every person I have encountered has had an unaccounted childhood history of abuse and/or sexual abuse. To me, this has been most notable among those who have had a long connection to the criminal justice system— namely African American men, and more specifically those who have endured long years in the foster care system.
After assessing over a thousand men who face lengthy prison sentences and endured long periods of solitary confinement, almost every person I have encountered has had an unaccounted childhood history of abuse and/or sexual abuse. To me, this has been most notable among those who have had a long connection to the criminal justice system— namely African American men, and more specifically those who have endured long years in the foster care system.
Many of the same patterns are also emerging within our immigration detention system, and so parallel conclusions can be applied to the immigrant population who are being held in prison-like settings. The goal of this article is to make the public aware of a growing epidemic of PTSD in our system of mass incarceration and detention. It calls for urgent attention to this immediate public health crisis. Addressing PTSD both in and out of correctional settings would lead to less violence and killings in prison and in the community.
The effects of living with untreated PTSD almost always flags a misdiagnosis of a mental health disorder of some other kind and no clinical account of the person’s abuse that can then lead to relevant basis for mitigation and the proper course for rehabilitation. It can also implicate mistreatment of symptoms and prescribing the wrong psychotropic medications to a person. In some instances, identifying PTSD can offer context to a whole host of other issues such as Traumatic Brain Injury (TBI), Depression, or co-occurring polysubstance abuse issues. Once PTSD is identified, it should lead to a long-term regimen of individual psychotherapy and addiction treatment where appropriate, with an emphasis on the mental health component. PTSD does not have to last forever but when it remains untreated, it can certainly last a lifetime.
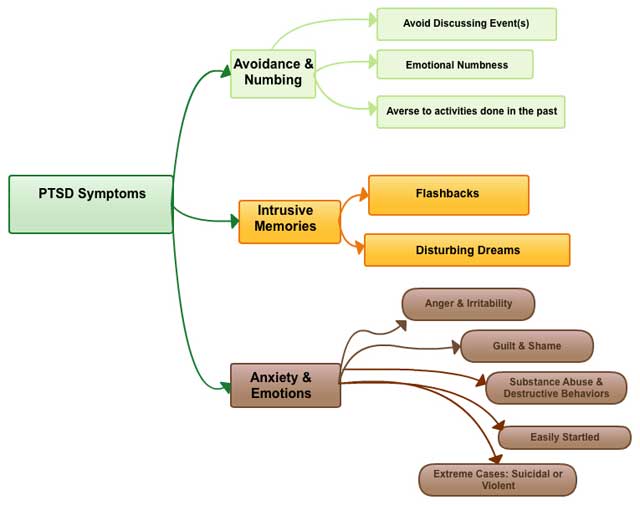
“Post Traumatic Stress Disorder (PTSD) is caused by both traumatic experiences before incarceration and institutional abuse during incarceration that includes the six clusters of symptoms: (1) intrusive memories and flashbacks to episodes of severe institutional abuse; (2) intense psychological distress and physiological reactivity when exposed to cues triggering memories of the institutional abuse; (3) episodes of dissociation, emotional numbing, and restricted affect; (4) chronic problems with mental functioning that include irritability, outbursts of anger, difficulty concentrating, sleep disturbances, and an exaggerated startle response. (5) persistent avoidance of anything that would trigger memories of the traumatic events; (6) hypervigilance, generalized paranoia, and reduced capacity to trust caused by constant fear of abuse from both correctional staff and other inmates that can be generalized to others after release,” according to Terence Gorski.
What Are Some Barriers to Identifying PTSD in Prisons and Detention Centers?
- A lack of basic trust between communities of color and mental health professionals who present themselves as affiliates of the system is pervasive among the prison population. Just within the past year, I met seven different incarcerated men who admitted to never disclosing their sexual abuse histories in previous psychological settings, largely due to feelings of distrust about disclosing personal information, deep shame, and feelings of worthlessness surrounding the abuse events. Indeed, an appropriate conversation about one’s traumatic histories leads one to be in his or her most vulnerable state. It requires a delicate process of assigning a substantive amount of time to assessing trauma between the interviewer and the person.
- Just the physical environment of a prison setting alone can deter an appropriate atmosphere for eliciting intimate information about one’s trauma history. Advocates, lawyers, social workers, and counselors may have to request appropriate accommodations within the prison to do a proper trauma assessment. It is always most ideal for the incarcerated person to feel as comfortable as possible before disclosing details of their past and present abuse. In many cases, this will not be possible and the one performing a trauma assessment has to decide whether it is appropriate for the person to be engaged in this type of interview. Conversations regarding trauma histories should be facilitated in a manner in which the person will not be re-traumatized while recounting past events.
- Proper training of correctional health staff, forensic health professionals, and legal advocates is necessary and critical. Those within correctional settings and the legal system should become a trauma-informed community to address the incarcerated population in a more realistic manner. Becoming a trauma-informed community will lead to less prison abuse and killings within correctional settings. Treating the root of an undetected problem will likely reduce recidivism among those that keep getting re-arrested and have long criminal histories.
- Cross-cultural biases may influence the interviewer to associate symptoms such as anger, hypervigilance, avoidance, or depressive symptoms of PTSD with other culturally and stereotypically held beliefs about men of color in the prison system. In addition, attributing the nature of the criminal charge against a person can cloud the belief that the incarcerated individual was also a victim of trauma in the past. This often leads many professionals to dismiss the likelihood that a client has a substantive abuse history.
- Even today’s well-trained lawyers and mental health advocates erroneously assume that if a person had an early history of trauma and abuse, it would have been documented a long time ago during an earlier course of treatment in previous years. This is an inaccurate assumption. It should be stressed that PTSD has only been truly understood among the medical community as recently as 2013 and this framework is not yet integrated within the legal and correctional system. Thus, the correctional and legal system largely still relies on outdated tools and outmoded diagnostic resources. Our historical pattern of under-treating PTSD among the incarcerated begs for a concerted effort and inquiry.
- Language barriers can also deter identifying PTSD when it exists. If the person is unable to speak English, it is critical that a trauma assessment is conducted and modified to the individual’s native language.
What We Can Do
Anyone who has had contact with the criminal justice system should be automatically considered predisposed to the conditions of PTSD and Complex PTSD. This assumption should be more pronounced among those who have been charged with a violent crime.
Becoming trauma-informed almost always requires a client-centered approach in either mental health or legal advocacy. It is absolutely essential that clients are put at ease, especially within prisons. Conducting trauma assessments almost always requires a skilled clinician who understands the continuum of PTSD and what its components look like. It is also important to allot an appropriate amount of time to acquire information related to one’s trauma history.
Commonly used universal screening tools in a proper trauma assessment are the PTSD Checklist (PCL-C) and the Life Events Checklist (LEC). To screen for signs of Traumatic Brain Injury or TBI, you can use the Harvard Trauma Questionnaire-Revised, a more developed cross-cultural tool to assess one’s history of torture, severe head injuries, and other extreme life hardships. You can also use the Hopkins Symptom Checklist-25, to screen for depression and anxiety symptoms. You may want to also use the Beck Depression Inventory II (BDI II) to look for depression symptoms that frequently co-exist with PTSD when left untreated for a long period of time.
After conducting a trauma assessment, various relaxation and stress reduction techniques can be taught to the one facing and enduring incarceration. An appropriate amount of follow-up should be done to see that the person is referred to proper treatment of PTSD for the long-run.


{kind=link}